Indications
Indications for the YAMIK Method are the following:
1. Acute exudative poly-sinusitis. Relapsing chronicle exudative poly-sinusitis. Acute exudative mono-sinusitis, mostly isolated ethmoiditis, sphenoiditis, frontal sinusitis (frontitis).
2. Preparation for surgery on the paranasal sinuses in patients with chronicle purulent and polypo-purulent sinusitis.
3. Recurrences of purulent sinusitis in patients who have undergone surgeries on the paranasal sinuses and endonasal structures.
1. Exudative mono-sinusitis or poly-sinusitis (acute or relapsing chronicle sinusitis). Yamik method is preferable when treating exudative mono-sinusitis and poly-sinusitis because when it’s applied ostiomeatal complex and affected nasal sinuses are treated directly and simultaneously. Yamik method effect achieved by comprehensive impact of guided pressure onto blood circulation in mucous membrane of nasal cavity results in reduction of mucous membrane edema and restoration of communicative function of epithelium. Certain significance is ascribed to changes in colloidal qualities of exudates in sinuses which become less viscous. Apart from affecting mucous membrane in nasal cavity in the ostiomeatal complex Yamik catheter enables:
- to drain out pathological secretion from sinuses;
- to introduce medication into the sinuses.
Introduction of appropriate medication into the paranasal sinuses enables to affect the impaired mucous membrane directly. This comprehensive impact eliminates such sinusitis symptoms as headaches, heavy nasal breathing and nasal discharge. And since blocked ostiomeatal complex and bacterial inflammation in paranasal sinuses are the main components of pathogenesis of acute and relapsing chronicle sinusitis, we regard it’s appropriate to declare the Yamik method a pathogenetic treatment method for this disease.
2. Preparation for surgery on the paranasal sinuses in patients with chronicle purulent and polypo-purulent sinusitis. When diagnosis is chronicle sinusitis it’s preferable to carry out surgery on the paranasal sinuses within a spell when there isn’t a purulent inflammation. Otherwise if the mucous membrane is inflamed the surgery will be rather complicated by bleeding which might ignificantly extend the duration of the surgery and increase the risk of injuring vital structures. Optimal way to relief the inflammation in paranasal sinuses over pre-surgery period is appliance of Yamik method which will considerably reduce blood loss and lessen risk of complication.
3. Recurrences of purulent sinusitis in patients who have undergone surgeries on the paranasal sinuses and endonasal structures. A surgery on paranasal sinuses and endonasal structures however efficiently accomplished will not secure a patient against recurrences of purulent sinusitis in future. There are dozens factors which can cause sinusitis including a common viral respiratory infection, general immunity decrease, allergic reaction and exposure to harmful environmental agents. Yamik method proved to be the best way to treat purulent inflammatory process in paranasal sinuses occurred after a surgery is carried out. Yamik method efficiency in stopping sinusitis relapse is conditioned by the fact that canals of paranasal sinuses are opened after the endonasal surgery. Thus sinuses can be easily drained from pathologic secretion and filled with appropriate medication.
Contra-indications
Contra-indications of the Yamik method are the following:
1. Old age
2. Purpura rheumatica
Yamik method procedure
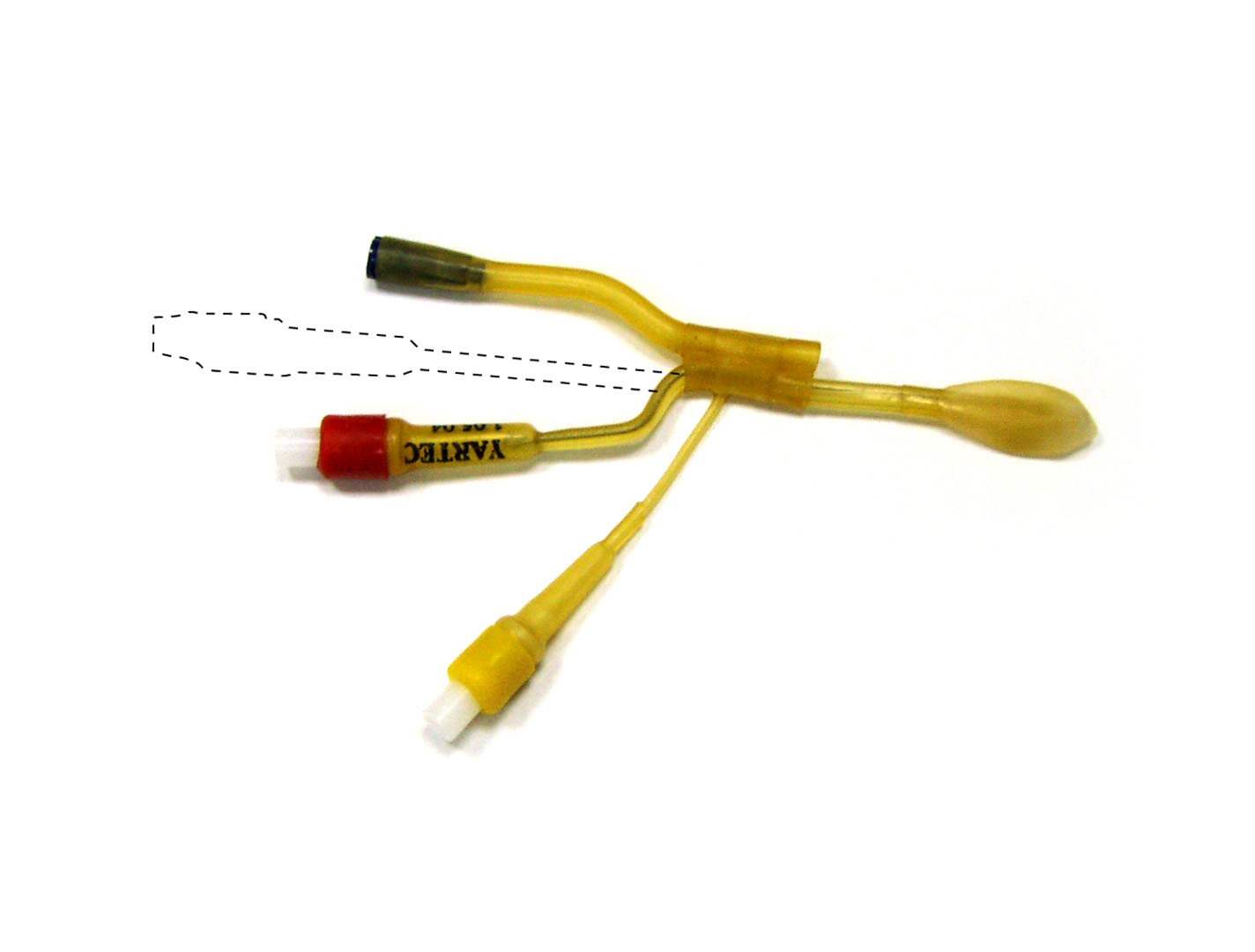
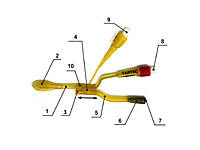
1. Design of sinus catheter Yamik-321 (Fig.1) Sinus catheter Yamik-321 consists of the main tube or central body (1) and a movable cuff (10). The structure of the central body includes a balloon (posterior balloon) (2) used to block the rhinopharynx and fitted with a valve (8) through which the air required to inflate the balloon is introduced. Inside the central body there is a semi-rigid metal core which allows altering the catheter’s shape.
 |
| Fig.1 |
 |
| Fig.2 |
 |
| Fig.3 |
Movable cuff consists of a balloon (anterior balloon) (4) used to isolate the vestibule from the nasal cavity and fitted with a valve (9) for its inflating.
The cuff is also linked with a working passage (6) which has internal (3) and external (7) openings. The external opening is fitted with an adapter to apply a syringe.
2. Tools kit necessary for the procedure To carry out the Yamik procedure the following tools must be available:
1. Sinus catheter Yamik-321
2. Rhinoscope
3. Spatula
4. Sprayer or probe with cotton wool coiled on it (for anesthesia procedure)
5. Syringe 20cc (to inflate the balloons)
6. Syringe 20cc (to drain out secretion from paranasal sinuses)
7. Syringe 20cc (to introduce medication into paranasal sinuses)
8. Solution for anesthesia (pantocaine 2% or other)
9. Adrenaline solution 1:1000 (0.1%)
3. Pre-usage preparation of the sinus catheter Yamik Sinus catheter Yamik is made of latex rubber so while preparing for the procedure it’s necessary to mind a number of certain conditions:
1. The procedure should be carried out at the temperature of no less than +15° C. In case the catheter was cooled it’s necessary before the procedure to place it in warm physiologic saline (+36° C).
 |
| Fig.4 |
 |
| Fig.5 |
2. Before applying the catheter it’s necessary to restore flexibility of the balloons:
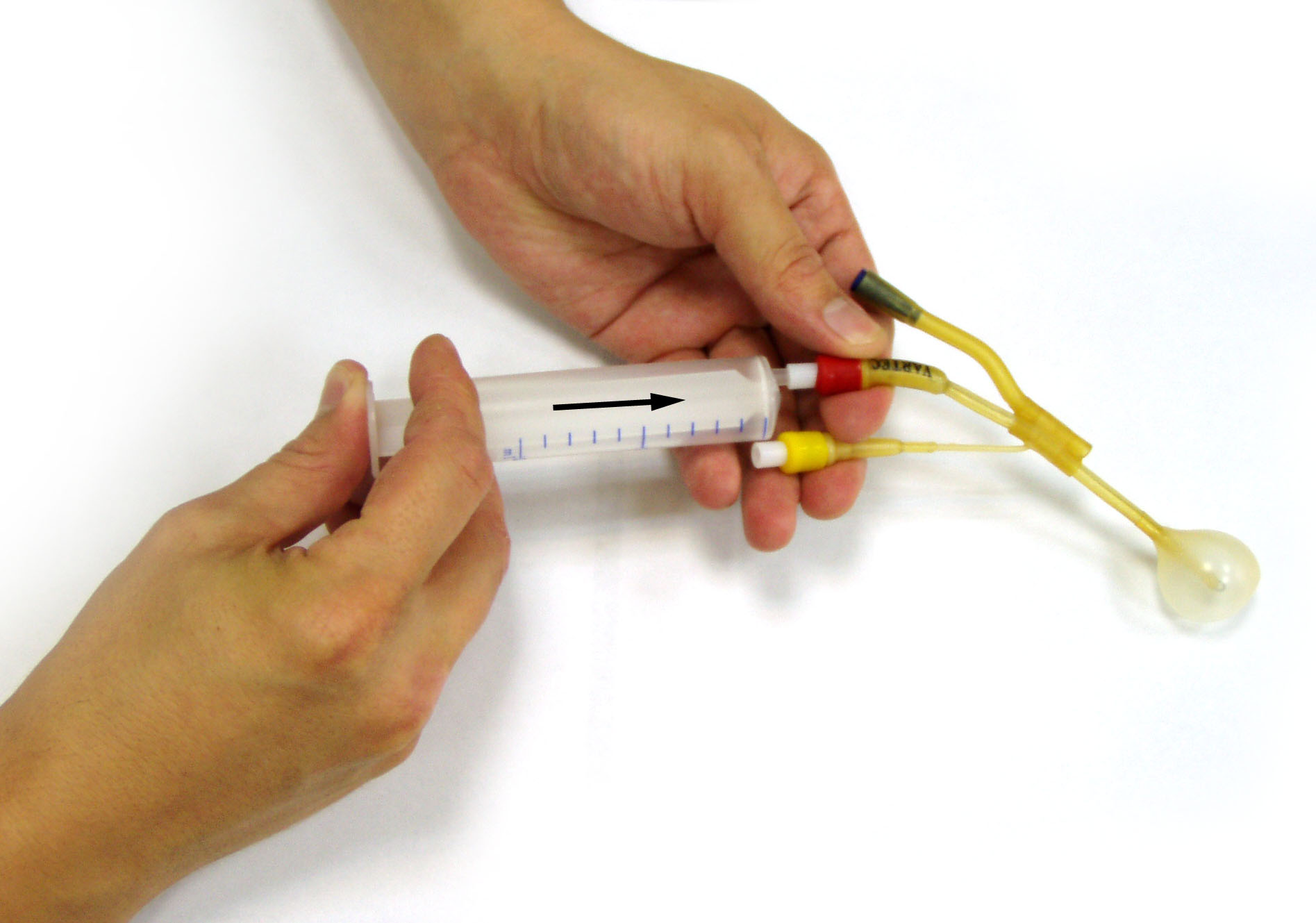
Step 1. Fill a syringe with air. Fit the syringe tip into the valve (8) push it slightly inside the valve and pressing the syringe piston fill the posterior balloon (2) with 6-7 cc of air (Fig.2)
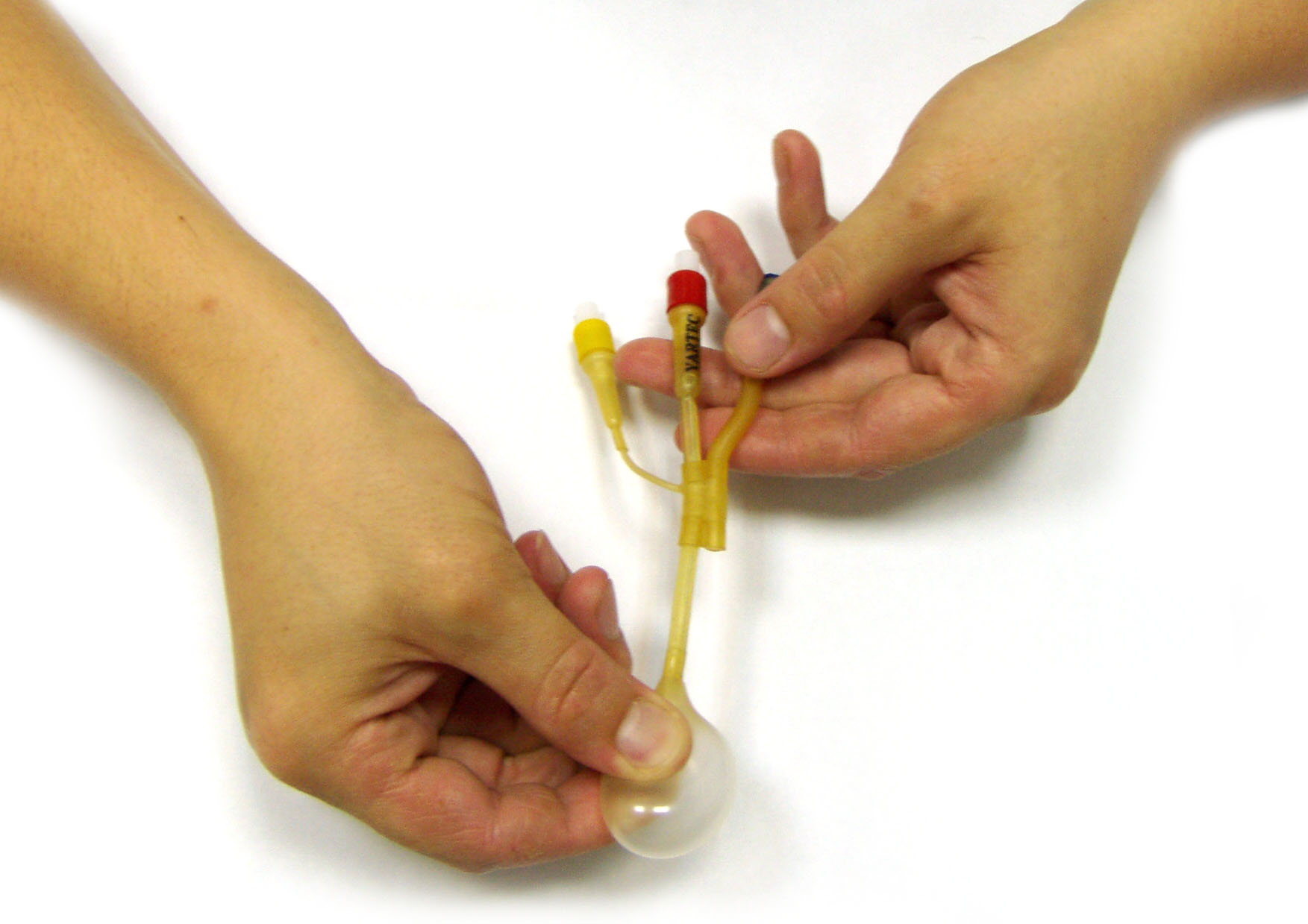
Step 2. Knead he balloon slightly with your fingers to make sure it’s uniforccy filled with air.
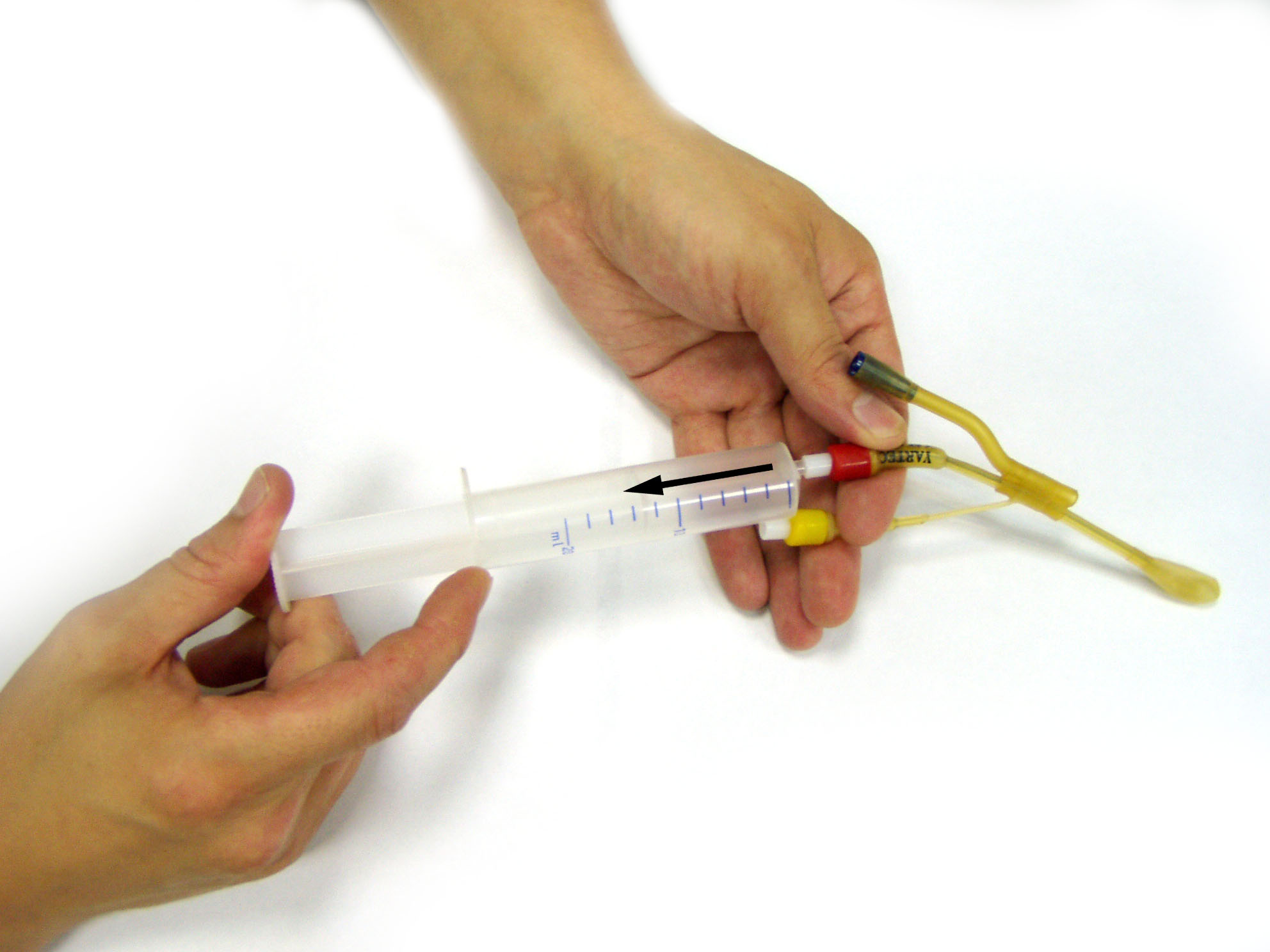
Step 3. Then It’s necessary to remove the air from the balloon. To do it fit the tip of the syringe into the valve (8) push it slightly inside the valve and by pulling the syringe piston back pump out the air. (Fig.4)
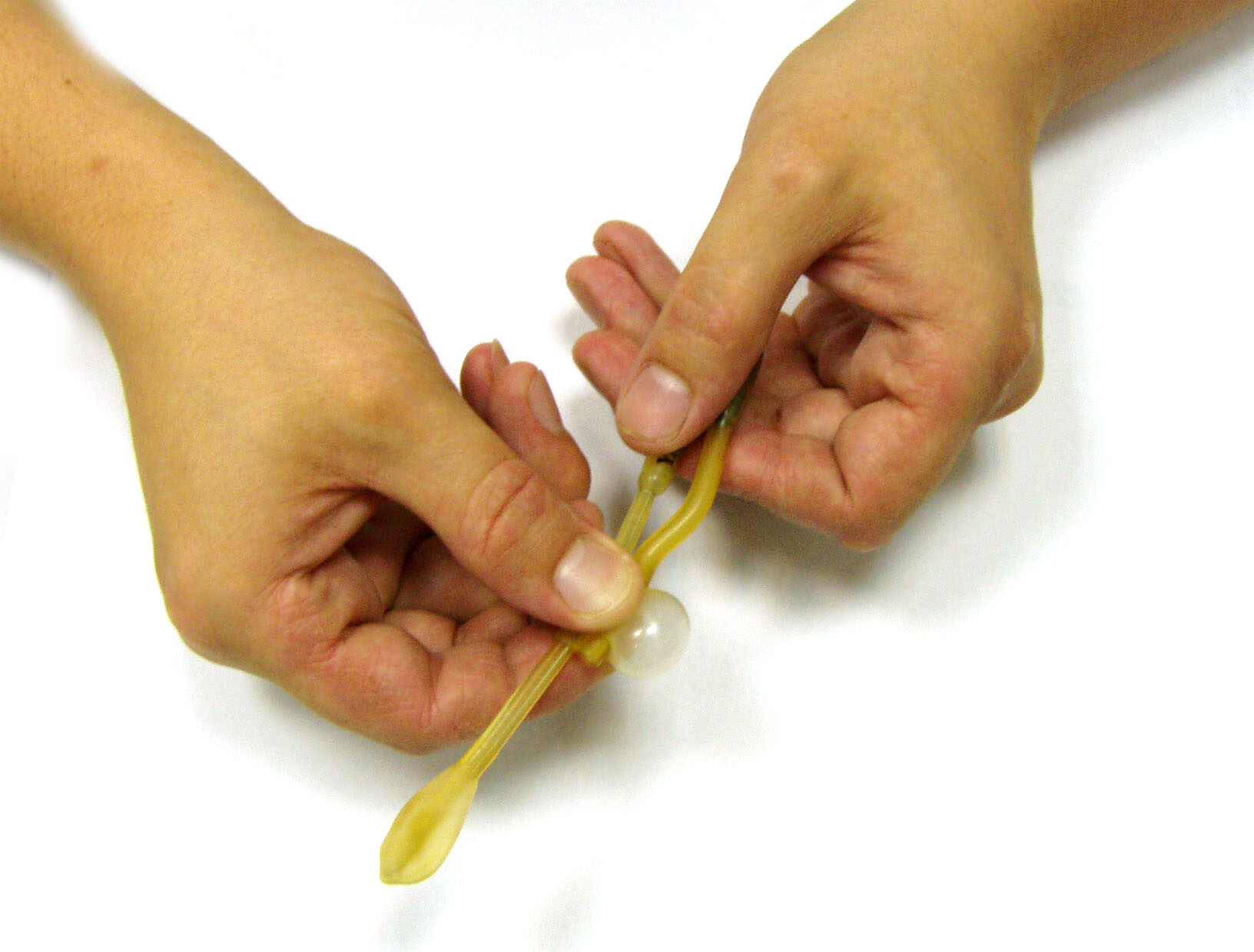
Step 4. Repeat the described procedure for the balloon on the movable cuff (4) thus inflating it by introducing 2-3cc of air through the valve (9).
4. Local anesthesia of nasal cavity mucous. First it’s necessary to apply vasoconstrictors to the nasal mucous membrane (particularly in the area of the middle nasal meatus). As vasoconstrictor 0.1% solution of adrenaline is recommended which can be applied to the mucous membrane of the middle nasal meatus either with the help of a probe with cotton wool or a cotton wool tampon introduced in the middle nasal meatus for 1-2 minutes.
 |
| Fig.6 |
To carry out the Yamik procedure it is necessary to administer local anesthesia of those areas of the nasal cavity and rhinopharynx mucous membrane which are supposed to contact with the balloons and the catheter main tube. It means that the anesthesia is to be applied to the mucous membrane of the front and rear sections of the nasal septum, lower part of the common nasal meatus and the fornix of the rhinopharynx. To apply anesthesia one can use either a probe with cotton wool or a sprayer(fig.6). In case the Yamik procedure is to be carried out on the both sides vasoconstrictor and anesthesia should be applied to the both sides simultaneously. The time of anesthesia action is determined by the qualities of the used anesthetic agent which are described in the annotation.
After vasoconstrictors are applied and local anesthesia is administered you can install the sinus-catheter in the nasal cavity.
5. Introduction (installation) of the sinus catheter Yamik into the patient’s nasal cavity. To carry out the Yamik procedure it is particularly significant to install the catheter into the nasal cavity in a proper way. Efficient introduction of the catheter is insured by the following conditions:
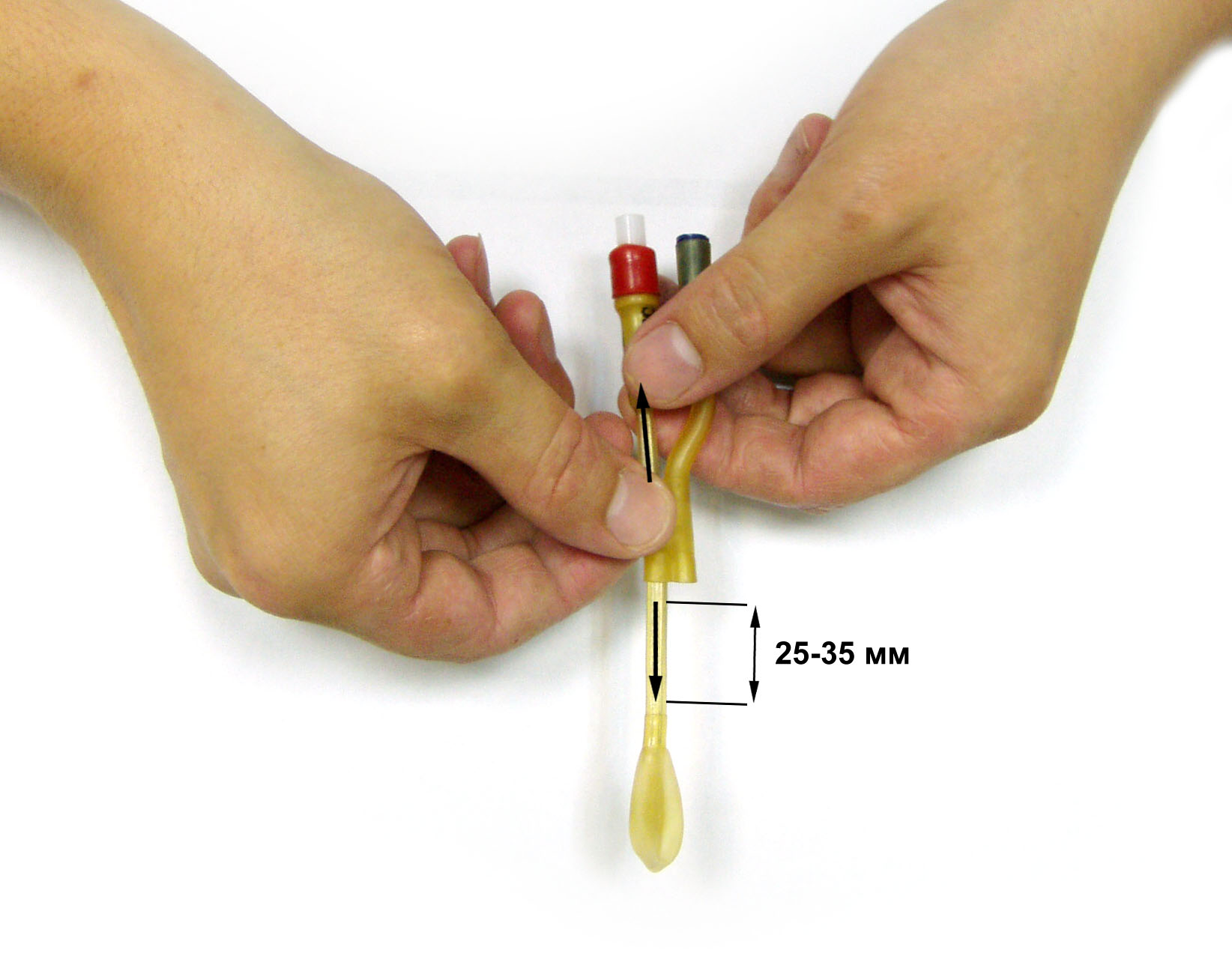
- correctly chosen distance between the balloons;
Step1. The distance between the balloons can be regulated with the help of the cuff (10) which is moved along the main tube (1) of the catheter (fig.7). For most patients optimal distance between the spot where the posterior balloon (2) is fastened to the central body of the catheter to the inside opening of the working passage (3) is as a rule 25mm.
- appropriate quantity of the air introduced into the balloons.
 |
| Fig.7 |
 |
| Fig.8 |
To fasten the cuff (10) securely in the needed position it is necessary to bend the catheter core right behind the cuff. Note that the core should be bent the way it’s shown at the fig.8. In cases when a patient has a “long” nasal meatus the distance between the balloons can be increased up to 30-35mm. The patient is in a seated position. The properly prepared catheter (fig.8) under control of the anterior rhinoscopy is introduced into the nasal cavity along the floor of the general nasal meatus parallel to the lower nasal turbinate (concha nasalis). Make the catheter slide along until the cuff is fitted in the vestibule of the nasal cavity (fig.9).
Step2. The rear balloon(2) which is installed in the rhinopharynx (pars nasalis pharynges) is then inflated with air through the valve (8) with the help of a 20cc syringe. For women and children the rear balloon (2) is filled with 8cc of air and for man the air amount is increased to 12 cc. (fig.10). After introducing the air into the balloon remove the syringe from the valve (8).
 |
| Fig.9 |
 |
| Fig.10 |
 |
| Fig.10a |
It is necessary to control the patient’s state and sensations since in some cases the amount of introduced air should be reduced. During the procedure it is crucial to hold the main body of the catheter because otherwise if exceedingly inflated the rear balloon can fall down into the oropharyngea (fig.10a). Next fit in the syringe tip into the valve (9) and inflate the cuff balloon (4) which is installed in the nasal vestibule (fig.10b).
The air amount necessary to inflate the cuff balloon (4) can vary and depends on the individual characteristics and size of the patient’s nasal cavity vestibule. The purpose of inflating the cuff balloon is to achieve complete occlusion of the nasal vestibule (fig.11 ). After all the above described actions have been carried out the sinus-catheter is supposed to be well fastened in the nasal cavity which allows you to proceed with the following stage.
6. Accomplishing the procedure For the procedure you’ll need a 20cc syringe. The patient remains in a seated position but with his/her head bent forwards and turned in the direction opposite to the nasal fossa into which the catheter was introduced. In this position the bottom of all the nasal sinuses is maximum higher than the fistulas, which facilitates drainage of any pathological discharge (substance)(fig.12).
 |
| Fig.10b |
 |
| Fig.11 |
 |
| Fig.12 |
A 20cc syringe is connected to the end of the working passage (6). The piston of the syringe must be positioned on the mark corresponding to 10cc (fig.13).
Make sure the catheter is fastened hermetically. Check hermiticity by pulling the syringe piston if the catheter is fastened tightly the skin of the nose wing should be pulled inside a bit lower the front edge of the piriform opening (apertura piriformis)(fig. 14).
In case hermiticity is achieved move the syringe piston forwards and backwards (fig.15). This will create a positive and negative pressure in the nasal cavity and the paranasal sinuses. It’s been proved that piston sliding inside the syringe body within the range between the two marks corresponding to 6 and 14cc causes a pressure of +/- 10-15 milibars inside the nasal cavity and paranasal sinuses. Practice shows that any changes in speed and amplitude of the piston sliding have no effect on the result of the procedure.
Piston sliding must be smooth without any jerks.
Creation of negative pressure inside the nasal cavity will determine aspiration first into the nasal cavity and then through the working passage into the syringe of any exudates present in the paranasal sinuses(fig.16).
 |
| Fig.13 |
 |
| Fig.14 |
 |
| Fig.15 |
The pathological substance is drained from the sinuses during 2 minutes.
This time is normally enough for complete and efficient drainage of the exudates. However if the exudates has not stopped coming into the syringe, the drainage procedure should be prolonged until the secretion stops coming into the syringe. If during 2 minutes no secretion starts coming out into the syringe, intermittent pressure should be stopped. It means that either the sinus fistulas are blocked or there’s no exudate in the sinuses. After that make the patient lie on his side with his/her head lying on the side of the affected sinuses, this position is optimal because the sinus fistulas are higher than the sinus bottom(fig.17).
Connect the tip of the syringe containing therapeutic solution to the entrance of the working passage(6).(Fig.18) Introduce a first portion of the solution
into the nasal cavity by pushing the syringe piston. The first portion should not be more than 1cc. Then the piston of the syringe is withdrawn in order to suck out the air from the sinuses. Air bubbles will be noticeable inside the syringe (fig.19). Keep on moving the syringe piston forwards and backwards which will build a negative pressure in nasal sinuses thus enabling the solution to penetrate easily into them. As a result the sinuses are filled with the solution.
 |
| Fig.16 |
 |
| Fig.17 |
 |
| Fig.18 |
Make sure you avoid exceeding positive pressure (syringe piston is moved forwards) cause it can push the solution into the oropharyngea. If the solution stopped coming from the syringe into the nasal cavity, it means that all the air in the sinuses was replaced with the medical solution.
The precise amount of the introduced solution should be carefully registered. Here the procedure is finished. Use the syringe to release the air from the balloons through the valves (8) and (9). First release the air from the posterior balloon (2) and then from anterior one (4). Carefully take the catheter out from the nose.
7. Peculiarities of Yamik method for children patients. Yamik method procedure for children patients is very similar to the one for adult patients, but there are certain peculiarities which are to be taken in consideration. In case of adult patients to block the rhinopharynx the posterior balloon of the sinus catheter should be filled with no less than 10-12 cc of air, whereas in cases with children patients the amount of air necessary to block the choanae from the side of the rhinopharynx is determined by the age of the child. Thus if the child is in 5-8 age category the air amount to fill the posterior balloon is no more than 6-8cc, and for children of 8-14 years of age the air amount increases up to 8-10cc. Before installing the catheter it is recommended to get the child patient psychologically ready for the procedure to avoid or reduce any negative response which might be expected from the child. The doctor explains to the child that the procedure is necessary and painless and shows him the sinus catheter and how the balloons are inflated. Active involvement of the child patient into the procedure turns the medical treatment process into a game thus suppressing the patient’s fear and reducing the pain reaction. It’s not accidental that among the children patients the Yamik procedure is known as “Balloons Inflating Game”.
 |
| Fig.19 |
8. Use of sinus catheter Yamik for sample extraction from paranasal sinuses for research and testing. In scientific and generally clinical purposes it is sometimes necessary to extract some material from the nasal cavity and paranasal sinuses for its examination and various types of research (bacteriolytic, immunological, cytological and other research purposes). This material might be the lavage from the whole mucous membrane of the nasal cavity and paranasal sinuses. First the catheter is installed in the nasal cavity and pathological secretion is drained from the paranasal sinuses. Then the sinuses are filled with 5-6cc of sterile physiologic saline which is then immediately drained back into the syringe. The received lavage can be used in required researches.
9. Recommendations. To achieve steady therapeutic efficacy there might be required from 2 to 6 Yamik procedures and in most cases it normally takes 3-4 procedures. Recommended frequency of the procedures is as following: First and second procedures are carried out in a sequence daily and two other procedures are done every other day.
In 90% cases during the first procedure the pathological secretion is drained from the sinuses and successfully replaced with medication. But it should be noted that in 10% cases pathological secretion is not drained out over the first procedure. But it doesn’t imply that the procedure hasn’t been efficient. As a rule a few hours after the procedure patients notice a considerable increase in amount of discharge from nasal cavity. It signifies that draining function of epithelia is being normalized.
It’s not indispensable to get exudates during the very first procedure. If exudate hasn’t been drained out it is necessary to warn the patient that there might be spontaneous draining of discharge from nasal sinuses a few hours after the procedure. In cases when cavity hasn’t been evacuated from secretion it is worthwhile to carry out the second procedure as soon as possible (for example on the next day). Treatment can be carried out either on an outpatient or inpatient basis depending on severity degree of sinusitis. Systemic antibiotic therapy is also proscribed as required. In most cases local applying of antibacterial solution by introducing it into paranasal sinuses is quite sufficient. One of Yamok method advantages is the possibility to control the course of treatment. The amount of medical solution introduced into the paranasal sinuses allows to assess the size of the sinuses (condition of the mucous membrane of the sinuses, presence of any secretion) and functioning of their natural fistulas. It should be noted that during the first two sessions it takes about one minute to introduce even a small amount of medical solution (2-3cc). Whereas at the end of the course of treatment it normally takes much less time: paranasal sinuses are filled with 10-12 cc of medical solution in as short time as 10-15seconds. Thus free and fast flow of the solution into the sinuses and filling up of the sinuses with 10-12 cc of solution can be an evidence to stopping of the sinusitis. Quite natural that diversity of anatomic peculiarities of nasal cavity shape makes it difficult to apply various medical tools and devices. Sinus catheter is not an exception in this respect. Followings are some of the problems one might face when using sinus catheters.
Practice shows that it’s impossible to insert a catheter into the nasal cavity if nasal septum is significantly distorted and the anterior nasal meatuses are not visible and can not be examined at anterior rhinoscopy. Another instance of the illness which makes it impossible and nonworthwhile to use the catheter is total nasal polyposis. One of the problems that may arise when carrying out treatment with the Yamic catheter occurs if it is impossible to create a negative pressure inside the nasal cavity and paranasal sinuses. This is due to incorrect positioning of the balloons. If the distance between the balloons is not properly defined there will be some space left between the inflated balloon and the walls of the nasal cavity. It is easy to notice any difficulty in creating a negative pressure in the nasal cavity when carrying out the aspiration movement with the piston of the syringe. If the problem occurred it is necessary to release the air from the balloons, remove the catheter from the nasal cavity and change the distance between the balloons. It might be necessary either to shorten the distance or to increase it by positioning the posterior balloon closer to the anterior balloon or moving it further from it respectively. Then the catheter is inserted again into the nasal cavity. If adequate closing of the nasal cavity is still not achieved, it will be necessary to ask the patient to say a few numbers out loud for example “one, two, three” and so on during the compression and decompression maneuvers. This will cause the soft palate to rise upwards enabling the nasal cavity to close by completing dorsally the function of posterior balloon. In most cases this method turns out to be efficient i.e. a negative pressure in the nasal cavity is built up which allows to carry out the treatment. Another problem that might occur during the Yamic procedure is building up of an excessive negative pressure. Specifically if this happens it will be impossible to withdraw the piston after fitting in the syringe tip to the working passage. This phenomenon can be explained by adhesion of the working passage opening to the mucous membrane of the nasal cavity. It happens due to deformation of the nasal septum (crests, spurs) or due to hypertrophy of the inferior nasal turbinate. If sensation of adhesion is experienced it is necessary to rotate the movable cuff of the catheter or to pull it slightly without releasing the air from the balloons, after that the treatment can be resumed. It should be mentioned that appearance of blood in the syringe during the Yamik procedure is an extremely rare case and can occur with doctors only starting mastering the use of the catheter. In case of hemorrhages the procedure must be stopped. The procedure should be carried out with extra precautions in patients with atrophic rhinitis and purpura rheumatica due to the risks of intense nasal hemorrhage which will require nasal packing. If the patient has a perforated nasal septum it will be necessary to use two sinus catheters at the same time. One of them will be inserted into the left half of the patient’s nose while the other will be applied on the right half. The end of the working passage of the catheter on the healthy side will have to be sealed with a small plug. The remaining part of the procedure will be no different from the usual manner in which it is performed.